First-trimester complications in pregnancy require careful sonographic evaluation for timely...
Understanding Abnormal First Trimester Symptoms
D
Dannielle Joseph@danniellejoseph
1 / 10
1
of 10
First-Trimester Complications
When examining patients during the first trimester, sonographers must be vigilant for various pregnancy complications. About 15% of clinically recognized pregnancies end in spontaneous miscarriage, with the rate likely higher for early unrecognized pregnancies.
Vaginal bleeding, occurring in nearly 25% of early pregnancies, is the most common presentation for complications. While bleeding can sometimes be inconsequential (such as implantation bleeding), it may signal a serious problem, especially when accompanied by severe pain, uterine contractions, or a dilated cervix.
Early transvaginal ultrasound examination is beneficial for patients with concerning symptoms. The sonographer should carefully examine the uterine cavity for the presence of an embryo, fetal heartbeat, yolk sac, or retained products of conception.
Clinical Alert: When a patient presents with first-trimester bleeding accompanied by severe pain, uterine contractions, or a dilated cervix, the pregnancy is unlikely to progress, making immediate evaluation critical.
2
of 10
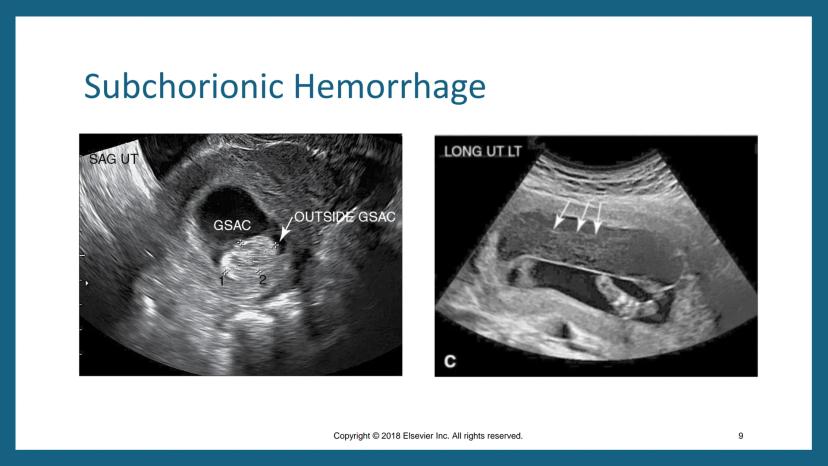
Subchorionic Hemorrhage
Subchorionic hemorrhage (SCH), also called subchorionic bleed, is the most common cause of first-trimester bleeding. This low-pressure bleed occurs during implantation of the fertilized ovum into the endometrial cavity and myometrial wall.
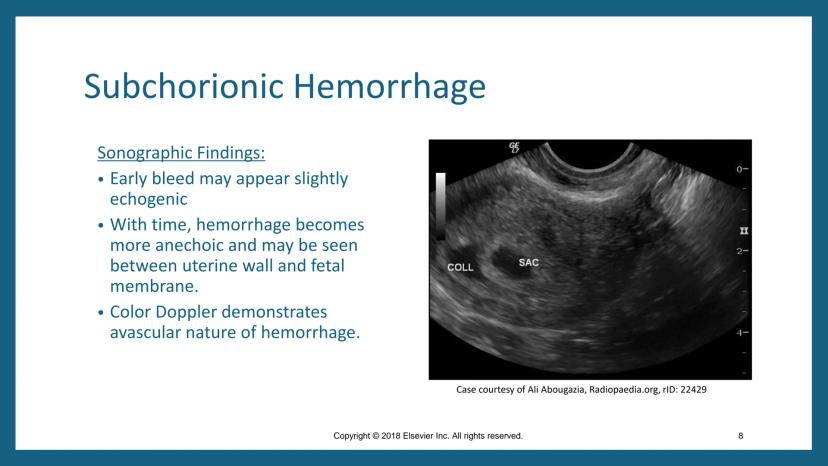
Sonographically, an SCH appears between the myometrium and margins of the gestational sac. Early bleeds may appear slightly echogenic, but with time, they become more anechoic and can be seen between the uterine wall and fetal membrane. Color Doppler helps demonstrate the avascular nature of the hemorrhage.
Patients may be asymptomatic or present with vaginal bleeding/spotting and uterine cramping. If the hemorrhage becomes large enough, it can lead to spontaneous abortion. This finding helps distinguish subchorionic hemorrhage from abruptio placentae, which generally occurs in the second trimester.
Remember: Color Doppler is an essential tool for confirming subchorionic hemorrhage by demonstrating its avascular nature, helping distinguish it from other vascular structures.
3
of 10
Spontaneous Abortion
When examining a patient with a potential spontaneous abortion, sonographers should look for visible embryonic parts, gestational sac, embryonic disc, or obvious evidence of retained products of conception. Sometimes distinguishing retained products from blood clots can be challenging.
Sonographic signs of retained products may be subtle, including a thickened endometrium (>8 mm) and increased vascularization of the endometrial complex. Color Doppler is strongly predictive in identifying this increased vascularization.
Quantitative hCG levels that don't decline normally, combined with sonographic findings, provide discriminating evidence for retained products. These findings guide clinical management decisions about whether intervention is needed.
Imaging Tip: When retained products are suspected but difficult to distinguish from blood clots, look for a thickened endometrium (>8 mm) combined with increased vascularization on Color Doppler for confirmation.
4
of 10
Anembryonic Pregnancy
An anembryonic pregnancy (also called blighted ovum) occurs when a gestational sac develops but the embryo fails to develop or stops developing at such an early stage that it's imperceptible by ultrasound. Trophoblastic tissue may continue to proliferate despite failed embryonic growth, causing the gestational sac to keep growing.
Sonographically, an anembryonic pregnancy typically appears as a large, empty gestational sac without a yolk sac, amnion, or embryo. In normal gestation, the mean sac diameter (MSD) increases by about 1 mm per day.
In subsequent repeat studies, the sonographer should evaluate growth size of the sac, presence of yolk sac, presence of embryo, measurement of embryo, and presence or absence of cardiac activity. These findings help confirm the diagnosis and guide management.
Key Diagnostic Point: When the mean sac diameter exceeds 18 mm without a visible embryo or exceeds 8 mm without a visible yolk sac, this strongly suggests an anembryonic pregnancy rather than an early normal gestation.
5
of 10
Pregnancy Failure
Sonographers need to be familiar with definitive signs of pregnancy failure. Findings that are diagnostic include: crown-rump length (CRL) ≥7 mm with no heartbeat, mean sac diameter (MSD) ≥25 mm with no embryo, or absence of embryo with heartbeat after appropriate waiting periods following earlier scans.
Suspicious but not diagnostic findings include: CRL <7 mm with no heartbeat, MSD 16-24 mm with no embryo, absence of embryo ≥6 weeks after last menstrual period, enlarged yolk sac >7 mm, or a small gestational sac in relation to the embryo.
Other indicators of pregnancy failure include an irregular or misshapen gestational sac, abnormal position (cornual, low, or hour-glassing through cervical os), slow or no growth, or hCG level discrepancy with sonographic findings.
Clinical Guideline: When findings are suspicious but not diagnostic of pregnancy failure, a follow-up scan in 7-10 days is recommended to avoid misdiagnosis of a potentially viable pregnancy.
6
of 10
Gestational Trophoblastic Disease
Gestational trophoblastic disease (GTD) is a spectrum of proliferative disorders of trophoblastic tissue after abnormal conception. It ranges from relatively benign forms like hydatidiform moles (partial, complete, or coexistent) to more malignant forms like invasive mole or choriocarcinoma.
Complete moles typically have no fetus, a normal diploid karyotype (46XX), and proliferating trophoblastic tissue without fetal development. Partial moles often show an abnormal fetus or fetal demise, a triploid karyotype (69XXY), and fetal parts may develop alongside abnormal trophoblastic tissue. Coexisting moles, which are rare, present as a normal fetus with normal placenta separate from a molar pregnancy.
Clinically, patients often present with vaginal bleeding in the first or early second trimester, dramatically elevated serum beta-hCG levels (often >100,000 IU/ml), and notably low maternal serum alpha-fetoprotein (MS-AFP). Other findings may include hyperemesis gravidarum, preeclampsia, bilateral adnexal fullness, and a uterus larger than expected for gestational age.
Laboratory Correlation: Dramatically elevated serum beta-hCG levels (often >100,000 IU/ml) combined with low maternal serum alpha-fetoprotein strongly suggest gestational trophoblastic disease rather than a normal pregnancy.
7
of 10
Sonographic Findings in Molar Pregnancy
The classic sonographic appearance of a hydatidiform mole is a "snowstorm" pattern - a moderately echogenic soft tissue mass filling the uterine cavity, marked with small cystic spaces representing hydropic chorionic villi. This gives the characteristic "cluster of grapes" appearance.
A complete mole shows no sign of a viable embryo, and may present with ovarian enlargement due to theca lutein cysts. A partial mole has identifiable placental tissue that is grossly enlarged and engorged with cystic spaces, and an embryo or embryonic tissue may be identified (though often abnormal).
The appearance of a first-trimester molar pregnancy may simulate other conditions including missed abortion, incomplete abortion, blighted ovum, or hydropic degeneration of placenta. This makes careful correlation with clinical and laboratory findings essential for diagnosis.
Differential Diagnosis: The "snowstorm" or "cluster of grapes" appearance on ultrasound is characteristic of molar pregnancy, but always correlate with extremely elevated hCG levels to differentiate from other conditions like missed abortion or hydropic degeneration.
8
of 10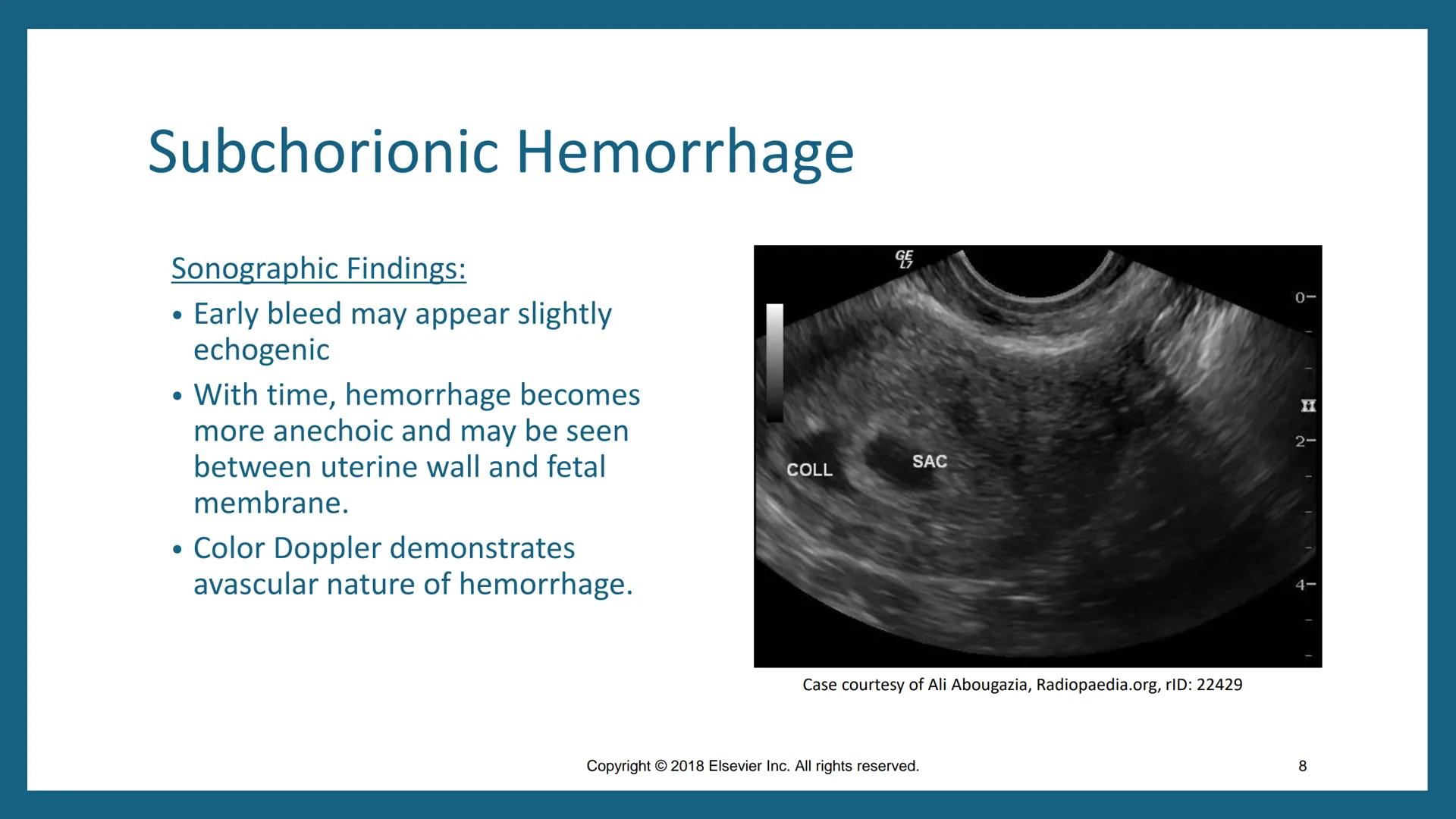
Abnormal or Absent Cardiac Activity
Identifying an intrauterine pregnancy with or without cardiac activity is the first conclusive sonographic sign of viability. The absence of cardiac activity in the first trimester is the most critical sign for determining pregnancy viability.
Technically, crown-rump length (CRL) ≥4 mm should demonstrate cardiac function. If an embryo is visible by sonography but cardiac activity cannot be documented, the prognosis is poor. Images should be made with the highest possible transducer frequency for maximum accuracy.
The sonographer should very carefully sweep the transducer through the gestational sac to image the embryo, cardiac motion, and yolk sac. Once cardiac activity is seen, M-mode should be used to record the actual heart rate. If any doubt exists in measurement, the patient should be reexamined in several days.
Technical Tip: When assessing embryonic cardiac activity, use M-mode to document heart rate precisely. An embryonic heart rate below 90 bpm at any gestational age within the first trimester indicates poor prognosis.
9
of 10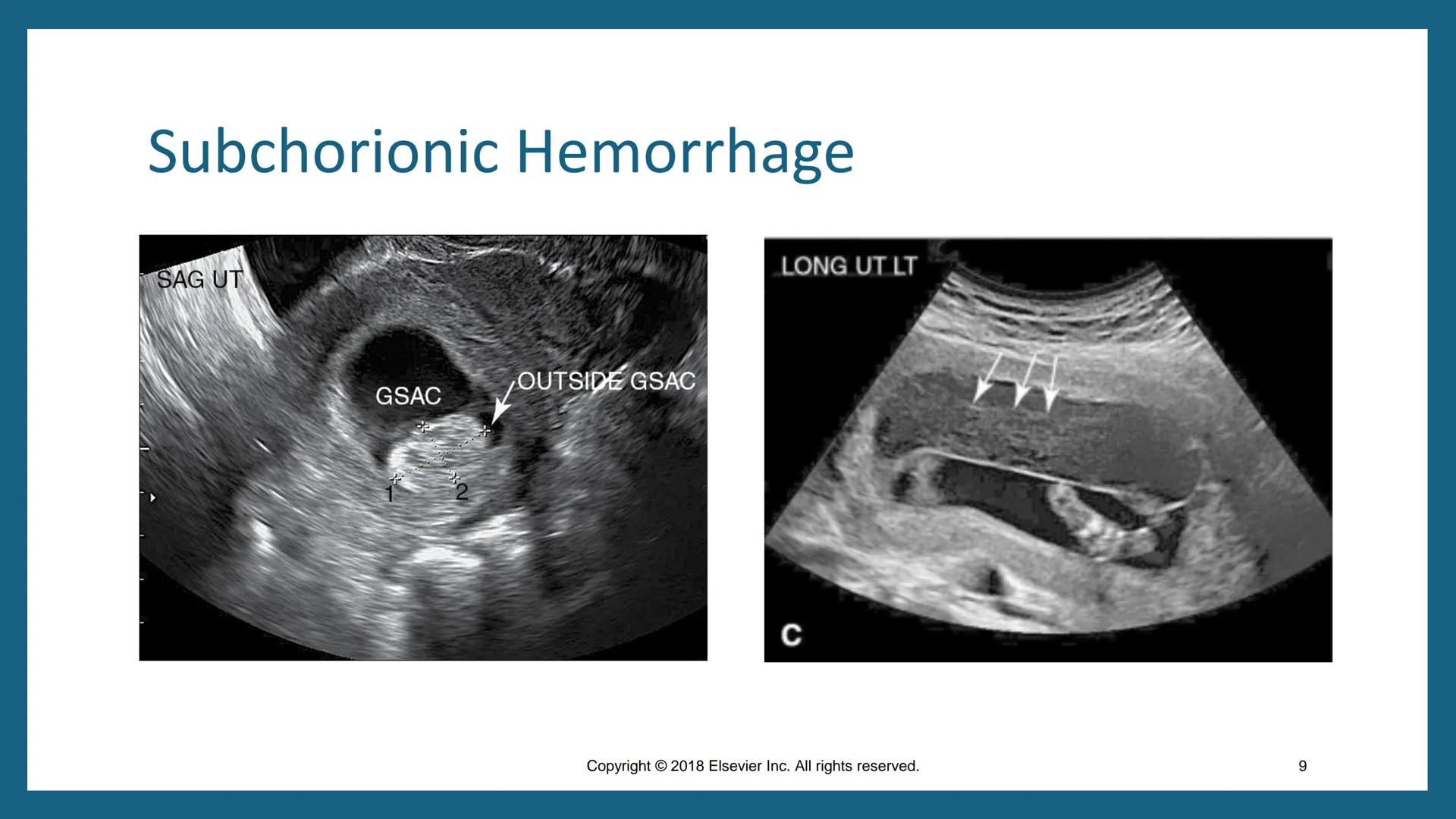
Embryonic Evaluations
The evaluation of embryonic structures provides valuable information about pregnancy viability. A normal yolk sac has expected growth of 0.3 mm/day with a maximal diameter of 5.5 mm between 5 and 10 weeks gestation. An enlarged yolk sac (≥5.6 mm) indicates increased risk for spontaneous pregnancy loss.
The amnion is best visualized with transvaginal sonography between the fifth and seventh weeks as a "double bleb sign" - the simultaneous side-by-side appearance of amnion and yolk sac. The mean amniotic sac diameter should be approximately equal to crown-rump length, with the amnion appearing as the thinner of the two concentric structures.
Growth delay and oligohydramnios (when the difference between mean sac diameter and CRL is <5 mm) within the first trimester have poor outcomes and are associated with chromosomal abnormalities such as triploidy.
Prognostic Indicator: An enlarged yolk sac (≥5.6 mm) or abnormally shaped yolk sac are strong indicators of potential pregnancy failure, warranting close follow-up even if cardiac activity is present.
10
of 10
Ectopic Pregnancy
Ectopic pregnancy is one of the most emergent diagnoses made with sonography, accounting for approximately 10% of maternal deaths. It occurs when a pregnancy is located outside the central/fundal location of the uterus. Risk factors include previous pelvic infections, use of IUDs, fallopian tube surgeries, infertility treatments, and history of ectopic pregnancy.
About 95% of ectopic pregnancies occur within the fallopian tube, with other sites such as the ovary, broad ligament, peritoneum, cervix, and cornua accounting for the remaining cases. Cornual/interstitial ectopics carry an increased risk for massive hemorrhage with rupture that may lead to hysterectomy or even death.
Clinical findings of pain are nonspecific and may vary, but classic findings associated with ectopic pregnancy include vaginal bleeding, an empty uterus, presence of an adnexal mass, and a positive pregnancy test.
Life-Threatening Alert: Cornual/interstitial ectopic pregnancies carry the highest risk for massive hemorrhage among ectopic pregnancies due to the rich vascular supply in this region, potentially requiring emergency hysterectomy.
We thought you’d never ask...
Our AI companion is specifically built for the needs of students. Based on the millions of content pieces we have on the platform we can provide truly meaningful and relevant answers to students. But its not only about answers, the companion is even more about guiding students through their daily learning challenges, with personalised study plans, quizzes or content pieces in the chat and 100% personalisation based on the students skills and developments.
You can download the app in the Google Play Store and in the Apple App Store.
That's right! Enjoy free access to study content, connect with fellow students, and get instant help – all at your fingertips.
Similar Content
Most popular content in AP Biology
9I
Introduction to Biological Elements of Life
Practice identifying the essential elements including carbon, nitrogen, phosphorus, and sulfur that compose biological macromolecules.
9th1,7410
I
Introduction to Water Polarity and Bonding
Practice identifying partial charges and the chemical basis of hydrogen bond formation between polar water molecules.
9th8520
I
Introduction to Biological Macromolecules
Practice identifying the four classes of biological macromolecules and the dehydration synthesis reactions that form their covalent bonds.
9th5980
I
Introduction to Biological Macromolecules
Practice identifying the monomers and chemical compositions of carbohydrates, lipids, proteins, and nucleic acids in biological systems.
9th4480
I
Introduction to Cell Compartmentalization
Practice identifying how membrane-bound organelles increase surface area and facilitate specialized chemical reactions in eukaryotic cells.
9th3370
C
Components of the Plasma Membrane
Practice identifying the molecular structure of phospholipids, proteins, cholesterol, and carbohydrates within the fluid mosaic model.
9th2770
I
Introduction to Evidence of Evolution
Practice identifying fundamental concepts of common ancestry, including homologous structures, vestigial traits, and the fossil record.
9th2010
Bio 1000 Chapter 2 The Molecules of Cells
Cell Make up
College55611
F
Fundamentals of Cell Size and Surface Area
Practice calculating surface area-to-volume ratios and defining how these geometric constraints limit the maximum size of a functional biological cell.
9th1550
Most popular content
9O
Origins and Dynamics of the Columbian Exchange
Analyze the ecological and economic motivations behind the initial transfer of goods, people, and diseases between the Old and New Worlds.
9th3,1280
I
Introduction to Early Cultural Interactions
Analyze the initial social and religious encounters between Europeans, Africans, and Indigenous peoples in the colonial Americas.
9th2,7730
O
Origins of Ancient River Civilizations
Analyze the environmental factors and technological innovations that led to the rise of early states in Mesopotamia, Egypt, and the Indus Valley.
9th3,1870
M
Motivations for European Exploration
Analyze the economic, religious, and political factors that drove European powers to the Americas during the 15th and 16th centuries.
9th1,7780
F
Foundations of Ethical Guidelines in Research
Practice the core principles of the APA ethical code including informed consent, debriefing, and the role of Institutional Review Boards.
9th1,3360
I
Introduction to Native American Societies
Examine the diverse social, political, and economic structures of North American indigenous groups prior to European contact.
9th1,1100
I
Introduction to the Spanish Encomienda System
Explore the fundamental economic and social structures of the Spanish colonial system, focusing on the encomienda and the casta social hierarchy.
9th8890
I
Introduction to Biological Elements of Life
Practice identifying the essential elements including carbon, nitrogen, phosphorus, and sulfur that compose biological macromolecules.
9th1,7410
O
Origins of the Articles of Confederation
Practice identifying the motivations for a weak central government and the specific powers granted to the states under the first U.S. constitution.
9th9370
Students love us — and so will you.
4.6/5App Store
4.7/5Google Play
The app is very easy to use and well designed. I have found everything I was looking for so far and have been able to learn a lot from the presentations! I will definitely use the app for a class assignment! And of course it also helps a lot as an inspiration.
Stefan SiOS user
This app is really great. There are so many study notes and help [...]. My problem subject is French, for example, and the app has so many options for help. Thanks to this app, I have improved my French. I would recommend it to anyone.
Samantha KlichAndroid user
Wow, I am really amazed. I just tried the app because I've seen it advertised many times and was absolutely stunned. This app is THE HELP you want for school and above all, it offers so many things, such as workouts and fact sheets, which have been VERY helpful to me personally.
AnnaiOS user
Understanding Abnormal First Trimester Symptoms
D
Dannielle Joseph@danniellejoseph
First-trimester complications in pregnancy require careful sonographic evaluation for timely diagnosis and management. These complications range from bleeding issues to ectopic pregnancies and embryonic abnormalities. Understanding the sonographic findings associated with each complication is crucial for proper patient care.
1
of 10
Sign up to see the content. It's free!
- Access to all documents
- Improve your grades
- Join milions of students
First-Trimester Complications
When examining patients during the first trimester, sonographers must be vigilant for various pregnancy complications. About 15% of clinically recognized pregnancies end in spontaneous miscarriage, with the rate likely higher for early unrecognized pregnancies.
Vaginal bleeding, occurring in nearly 25% of early pregnancies, is the most common presentation for complications. While bleeding can sometimes be inconsequential (such as implantation bleeding), it may signal a serious problem, especially when accompanied by severe pain, uterine contractions, or a dilated cervix.
Early transvaginal ultrasound examination is beneficial for patients with concerning symptoms. The sonographer should carefully examine the uterine cavity for the presence of an embryo, fetal heartbeat, yolk sac, or retained products of conception.
Clinical Alert: When a patient presents with first-trimester bleeding accompanied by severe pain, uterine contractions, or a dilated cervix, the pregnancy is unlikely to progress, making immediate evaluation critical.
2
of 10Sign up to see the content. It's free!
- Access to all documents
- Improve your grades
- Join milions of students
Subchorionic Hemorrhage
Subchorionic hemorrhage (SCH), also called subchorionic bleed, is the most common cause of first-trimester bleeding. This low-pressure bleed occurs during implantation of the fertilized ovum into the endometrial cavity and myometrial wall.
Sonographically, an SCH appears between the myometrium and margins of the gestational sac. Early bleeds may appear slightly echogenic, but with time, they become more anechoic and can be seen between the uterine wall and fetal membrane. Color Doppler helps demonstrate the avascular nature of the hemorrhage.
Patients may be asymptomatic or present with vaginal bleeding/spotting and uterine cramping. If the hemorrhage becomes large enough, it can lead to spontaneous abortion. This finding helps distinguish subchorionic hemorrhage from abruptio placentae, which generally occurs in the second trimester.
Remember: Color Doppler is an essential tool for confirming subchorionic hemorrhage by demonstrating its avascular nature, helping distinguish it from other vascular structures.
3
of 10Sign up to see the content. It's free!
- Access to all documents
- Improve your grades
- Join milions of students
Spontaneous Abortion
When examining a patient with a potential spontaneous abortion, sonographers should look for visible embryonic parts, gestational sac, embryonic disc, or obvious evidence of retained products of conception. Sometimes distinguishing retained products from blood clots can be challenging.
Sonographic signs of retained products may be subtle, including a thickened endometrium (>8 mm) and increased vascularization of the endometrial complex. Color Doppler is strongly predictive in identifying this increased vascularization.
Quantitative hCG levels that don't decline normally, combined with sonographic findings, provide discriminating evidence for retained products. These findings guide clinical management decisions about whether intervention is needed.
Imaging Tip: When retained products are suspected but difficult to distinguish from blood clots, look for a thickened endometrium (>8 mm) combined with increased vascularization on Color Doppler for confirmation.
4
of 10Sign up to see the content. It's free!
- Access to all documents
- Improve your grades
- Join milions of students
Anembryonic Pregnancy
An anembryonic pregnancy (also called blighted ovum) occurs when a gestational sac develops but the embryo fails to develop or stops developing at such an early stage that it's imperceptible by ultrasound. Trophoblastic tissue may continue to proliferate despite failed embryonic growth, causing the gestational sac to keep growing.
Sonographically, an anembryonic pregnancy typically appears as a large, empty gestational sac without a yolk sac, amnion, or embryo. In normal gestation, the mean sac diameter (MSD) increases by about 1 mm per day.
In subsequent repeat studies, the sonographer should evaluate growth size of the sac, presence of yolk sac, presence of embryo, measurement of embryo, and presence or absence of cardiac activity. These findings help confirm the diagnosis and guide management.
Key Diagnostic Point: When the mean sac diameter exceeds 18 mm without a visible embryo or exceeds 8 mm without a visible yolk sac, this strongly suggests an anembryonic pregnancy rather than an early normal gestation.
5
of 10Sign up to see the content. It's free!
- Access to all documents
- Improve your grades
- Join milions of students
Pregnancy Failure
Sonographers need to be familiar with definitive signs of pregnancy failure. Findings that are diagnostic include: crown-rump length (CRL) ≥7 mm with no heartbeat, mean sac diameter (MSD) ≥25 mm with no embryo, or absence of embryo with heartbeat after appropriate waiting periods following earlier scans.
Suspicious but not diagnostic findings include: CRL <7 mm with no heartbeat, MSD 16-24 mm with no embryo, absence of embryo ≥6 weeks after last menstrual period, enlarged yolk sac >7 mm, or a small gestational sac in relation to the embryo.
Other indicators of pregnancy failure include an irregular or misshapen gestational sac, abnormal position (cornual, low, or hour-glassing through cervical os), slow or no growth, or hCG level discrepancy with sonographic findings.
Clinical Guideline: When findings are suspicious but not diagnostic of pregnancy failure, a follow-up scan in 7-10 days is recommended to avoid misdiagnosis of a potentially viable pregnancy.
6
of 10Sign up to see the content. It's free!
- Access to all documents
- Improve your grades
- Join milions of students
Gestational Trophoblastic Disease
Gestational trophoblastic disease (GTD) is a spectrum of proliferative disorders of trophoblastic tissue after abnormal conception. It ranges from relatively benign forms like hydatidiform moles (partial, complete, or coexistent) to more malignant forms like invasive mole or choriocarcinoma.
Complete moles typically have no fetus, a normal diploid karyotype (46XX), and proliferating trophoblastic tissue without fetal development. Partial moles often show an abnormal fetus or fetal demise, a triploid karyotype (69XXY), and fetal parts may develop alongside abnormal trophoblastic tissue. Coexisting moles, which are rare, present as a normal fetus with normal placenta separate from a molar pregnancy.
Clinically, patients often present with vaginal bleeding in the first or early second trimester, dramatically elevated serum beta-hCG levels (often >100,000 IU/ml), and notably low maternal serum alpha-fetoprotein (MS-AFP). Other findings may include hyperemesis gravidarum, preeclampsia, bilateral adnexal fullness, and a uterus larger than expected for gestational age.
Laboratory Correlation: Dramatically elevated serum beta-hCG levels (often >100,000 IU/ml) combined with low maternal serum alpha-fetoprotein strongly suggest gestational trophoblastic disease rather than a normal pregnancy.
7
of 10Sign up to see the content. It's free!
- Access to all documents
- Improve your grades
- Join milions of students
Sonographic Findings in Molar Pregnancy
The classic sonographic appearance of a hydatidiform mole is a "snowstorm" pattern - a moderately echogenic soft tissue mass filling the uterine cavity, marked with small cystic spaces representing hydropic chorionic villi. This gives the characteristic "cluster of grapes" appearance.
A complete mole shows no sign of a viable embryo, and may present with ovarian enlargement due to theca lutein cysts. A partial mole has identifiable placental tissue that is grossly enlarged and engorged with cystic spaces, and an embryo or embryonic tissue may be identified (though often abnormal).
The appearance of a first-trimester molar pregnancy may simulate other conditions including missed abortion, incomplete abortion, blighted ovum, or hydropic degeneration of placenta. This makes careful correlation with clinical and laboratory findings essential for diagnosis.
Differential Diagnosis: The "snowstorm" or "cluster of grapes" appearance on ultrasound is characteristic of molar pregnancy, but always correlate with extremely elevated hCG levels to differentiate from other conditions like missed abortion or hydropic degeneration.
8
of 10Sign up to see the content. It's free!
- Access to all documents
- Improve your grades
- Join milions of students
Abnormal or Absent Cardiac Activity
Identifying an intrauterine pregnancy with or without cardiac activity is the first conclusive sonographic sign of viability. The absence of cardiac activity in the first trimester is the most critical sign for determining pregnancy viability.
Technically, crown-rump length (CRL) ≥4 mm should demonstrate cardiac function. If an embryo is visible by sonography but cardiac activity cannot be documented, the prognosis is poor. Images should be made with the highest possible transducer frequency for maximum accuracy.
The sonographer should very carefully sweep the transducer through the gestational sac to image the embryo, cardiac motion, and yolk sac. Once cardiac activity is seen, M-mode should be used to record the actual heart rate. If any doubt exists in measurement, the patient should be reexamined in several days.
Technical Tip: When assessing embryonic cardiac activity, use M-mode to document heart rate precisely. An embryonic heart rate below 90 bpm at any gestational age within the first trimester indicates poor prognosis.
9
of 10Sign up to see the content. It's free!
- Access to all documents
- Improve your grades
- Join milions of students
Embryonic Evaluations
The evaluation of embryonic structures provides valuable information about pregnancy viability. A normal yolk sac has expected growth of 0.3 mm/day with a maximal diameter of 5.5 mm between 5 and 10 weeks gestation. An enlarged yolk sac (≥5.6 mm) indicates increased risk for spontaneous pregnancy loss.
The amnion is best visualized with transvaginal sonography between the fifth and seventh weeks as a "double bleb sign" - the simultaneous side-by-side appearance of amnion and yolk sac. The mean amniotic sac diameter should be approximately equal to crown-rump length, with the amnion appearing as the thinner of the two concentric structures.
Growth delay and oligohydramnios (when the difference between mean sac diameter and CRL is <5 mm) within the first trimester have poor outcomes and are associated with chromosomal abnormalities such as triploidy.
Prognostic Indicator: An enlarged yolk sac (≥5.6 mm) or abnormally shaped yolk sac are strong indicators of potential pregnancy failure, warranting close follow-up even if cardiac activity is present.
10
of 10Sign up to see the content. It's free!
- Access to all documents
- Improve your grades
- Join milions of students
Ectopic Pregnancy
Ectopic pregnancy is one of the most emergent diagnoses made with sonography, accounting for approximately 10% of maternal deaths. It occurs when a pregnancy is located outside the central/fundal location of the uterus. Risk factors include previous pelvic infections, use of IUDs, fallopian tube surgeries, infertility treatments, and history of ectopic pregnancy.
About 95% of ectopic pregnancies occur within the fallopian tube, with other sites such as the ovary, broad ligament, peritoneum, cervix, and cornua accounting for the remaining cases. Cornual/interstitial ectopics carry an increased risk for massive hemorrhage with rupture that may lead to hysterectomy or even death.
Clinical findings of pain are nonspecific and may vary, but classic findings associated with ectopic pregnancy include vaginal bleeding, an empty uterus, presence of an adnexal mass, and a positive pregnancy test.
Life-Threatening Alert: Cornual/interstitial ectopic pregnancies carry the highest risk for massive hemorrhage among ectopic pregnancies due to the rich vascular supply in this region, potentially requiring emergency hysterectomy.
We thought you’d never ask...
Our AI companion is specifically built for the needs of students. Based on the millions of content pieces we have on the platform we can provide truly meaningful and relevant answers to students. But its not only about answers, the companion is even more about guiding students through their daily learning challenges, with personalised study plans, quizzes or content pieces in the chat and 100% personalisation based on the students skills and developments.
You can download the app in the Google Play Store and in the Apple App Store.
That's right! Enjoy free access to study content, connect with fellow students, and get instant help – all at your fingertips.
Similar Content
Most popular content in AP Biology
9I
Introduction to Biological Elements of Life
Practice identifying the essential elements including carbon, nitrogen, phosphorus, and sulfur that compose biological macromolecules.
9th1,7410
I
Introduction to Water Polarity and Bonding
Practice identifying partial charges and the chemical basis of hydrogen bond formation between polar water molecules.
9th8520
I
Introduction to Biological Macromolecules
Practice identifying the four classes of biological macromolecules and the dehydration synthesis reactions that form their covalent bonds.
9th5980
I
Introduction to Biological Macromolecules
Practice identifying the monomers and chemical compositions of carbohydrates, lipids, proteins, and nucleic acids in biological systems.
9th4480
I
Introduction to Cell Compartmentalization
Practice identifying how membrane-bound organelles increase surface area and facilitate specialized chemical reactions in eukaryotic cells.
9th3370
C
Components of the Plasma Membrane
Practice identifying the molecular structure of phospholipids, proteins, cholesterol, and carbohydrates within the fluid mosaic model.
9th2770
I
Introduction to Evidence of Evolution
Practice identifying fundamental concepts of common ancestry, including homologous structures, vestigial traits, and the fossil record.
9th2010
Bio 1000 Chapter 2 The Molecules of Cells
Cell Make up
College55611
F
Fundamentals of Cell Size and Surface Area
Practice calculating surface area-to-volume ratios and defining how these geometric constraints limit the maximum size of a functional biological cell.
9th1550
Most popular content
9O
Origins and Dynamics of the Columbian Exchange
Analyze the ecological and economic motivations behind the initial transfer of goods, people, and diseases between the Old and New Worlds.
9th3,1280
I
Introduction to Early Cultural Interactions
Analyze the initial social and religious encounters between Europeans, Africans, and Indigenous peoples in the colonial Americas.
9th2,7730
O
Origins of Ancient River Civilizations
Analyze the environmental factors and technological innovations that led to the rise of early states in Mesopotamia, Egypt, and the Indus Valley.
9th3,1870
M
Motivations for European Exploration
Analyze the economic, religious, and political factors that drove European powers to the Americas during the 15th and 16th centuries.
9th1,7780
F
Foundations of Ethical Guidelines in Research
Practice the core principles of the APA ethical code including informed consent, debriefing, and the role of Institutional Review Boards.
9th1,3360
I
Introduction to Native American Societies
Examine the diverse social, political, and economic structures of North American indigenous groups prior to European contact.
9th1,1100
I
Introduction to the Spanish Encomienda System
Explore the fundamental economic and social structures of the Spanish colonial system, focusing on the encomienda and the casta social hierarchy.
9th8890
I
Introduction to Biological Elements of Life
Practice identifying the essential elements including carbon, nitrogen, phosphorus, and sulfur that compose biological macromolecules.
9th1,7410
O
Origins of the Articles of Confederation
Practice identifying the motivations for a weak central government and the specific powers granted to the states under the first U.S. constitution.
9th9370
Students love us — and so will you.
4.6/5App Store
4.7/5Google Play
The app is very easy to use and well designed. I have found everything I was looking for so far and have been able to learn a lot from the presentations! I will definitely use the app for a class assignment! And of course it also helps a lot as an inspiration.
Stefan SiOS user
This app is really great. There are so many study notes and help [...]. My problem subject is French, for example, and the app has so many options for help. Thanks to this app, I have improved my French. I would recommend it to anyone.
Samantha KlichAndroid user
Wow, I am really amazed. I just tried the app because I've seen it advertised many times and was absolutely stunned. This app is THE HELP you want for school and above all, it offers so many things, such as workouts and fact sheets, which have been VERY helpful to me personally.
AnnaiOS user